1- Introduction to Dental Esthetics and the Esthetic Zone
A- Esthetic Zone (Appearance Zone): It is the part of the mouth where high visibility requires a restoration or tooth replacement to simulate the natural appearance of a tooth.
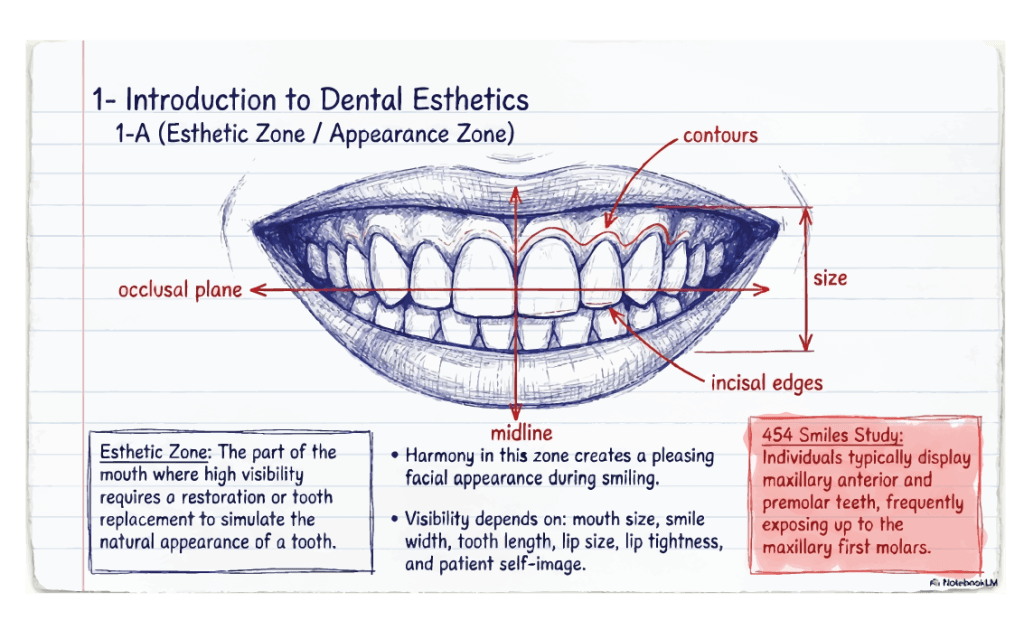
I- Harmony in this zone contributes to a pleasing facial appearance, particularly when the patient smiles.
II- Elements that must be in harmony include contours, size, incisal edges, occlusal plane, and the midline.
III- Visibility varies by individual depending on mouth size, smile width, tooth length, lip size, lip tightness, and the patient’s self-image.
IV- In a study of 454 smiles, individuals typically displayed maxillary anterior and premolar teeth, frequently including the maxillary first molars.
B- The Smile Line (Incisal Curve): It is a curve composed of the incisal edges of the maxillary anterior teeth that parallels the inner curvature of the lower lip.
I- The incisal curve should be perpendicular to the midline and parallel with the interpupillary axis. II- Nearly 80% of young subjects display the entire length of their maxillary anterior teeth. III- At rest, women typically show nearly twice as much of their maxillary central incisors as men (3.4 mm vs. 1.9 mm). IV- Men are 2.4 times more likely to have a low smile line than women.
C- Phonetic and Functional Considerations:
I- Maxillary incisor length cannot be established by esthetics alone as they play a critical role in anterior guidance and phonetics.
II- The “F” Sound: When sounding the letter “f,” the maxillary incisal edges should touch the inner edge of the vermilion border (the “wet-dry line”) of the lower lip.
III- The “S” Sound: When pronouncing the letter “s,” the incisal edges of the mandibular incisors are established by occlusal contact and a position 1.0 mm behind and 1.0 mm below the edges of the maxillary teeth.
D- Effects of Aging on Tooth Exposure:
I- As time and gravity affect the tissues surrounding the mouth, the length of exposed maxillary incisors diminishes. II- Conversely, the amount of visible mandibular incisor increases. III- At age 60, maxillary central incisor exposure below the lip is often 0.0 mm, while mandibular incisor exposure reaches nearly 3.0 mm.
2- Geometric and Mathematical Principles of Esthetics
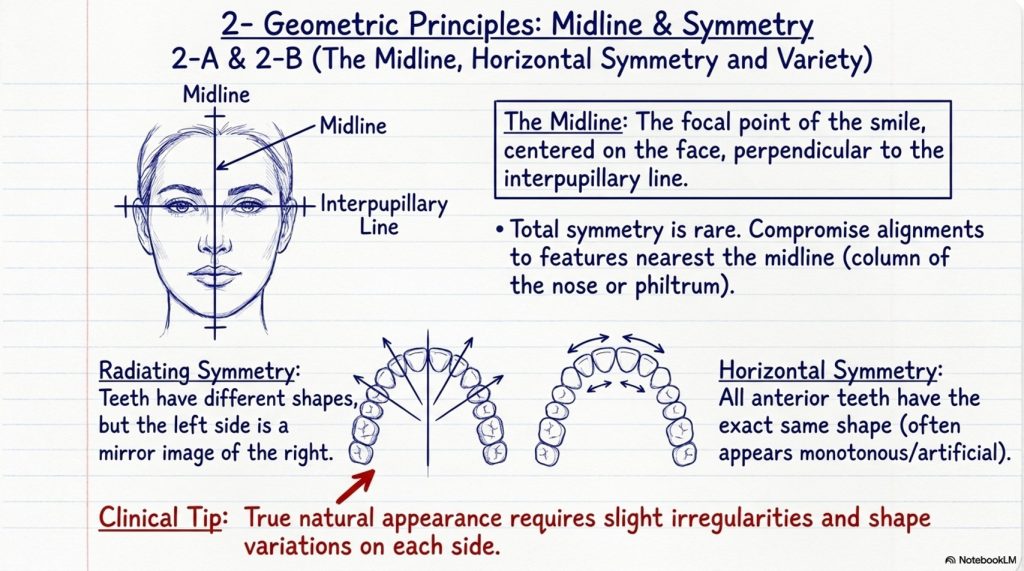
A- The Midline: It is the focal point of the smile, centered on the face and perpendicular to the interpupillary line.
I- Total symmetry is rare; if compromises are necessary, the midline should correspond to the features nearest to it, such as the column of the nose or the philtrum.
B- Horizontal Symmetry and Variety:
I- Radiating Symmetry: Results when teeth have different shapes but the left side is a mirror image of the right.
II- Horizontal Symmetry: Occurs when all anterior teeth have the same shape; this is often considered monotonous and artificial.
III- A natural appearance is produced by introducing slight irregularities and variations in arrangement and shape to each side.
C- The Golden Proportion (Divine Proportion):
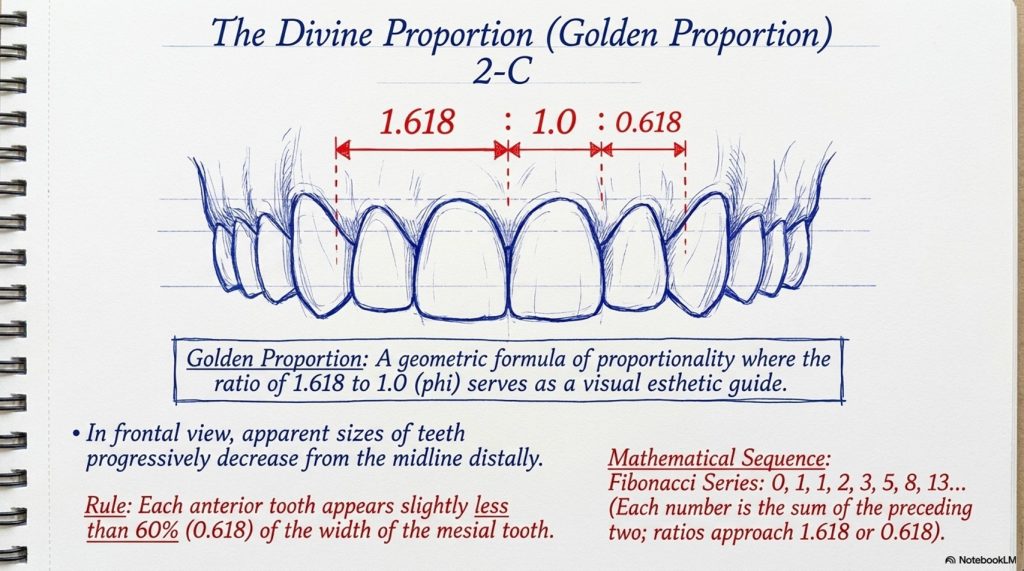
It is a geometric formula of proportionality where the ratio of 1.618 to 1.0 (phi) serves as a guide for visual esthetics.
I- In a frontal view, the apparent sizes of teeth should become progressively smaller from the midline distally.
II- Each anterior tooth should appear slightly less than 60% (0.618) of the width of the tooth immediately mesial to it.
III- Fibonacci Series: A sequence of numbers (0, 1, 1, 2, 3, 5, 8, 13…) where each number is the sum of the preceding two; their ratios approximate 1.618 or 0.618 as the numbers increase.
D- Tooth Alignment and Morphology:
I- The long axes of maxillary incisor crowns should converge slightly toward the midline.
II- The long axes of the crowns of posterior teeth are inclined toward the lingual.
III- Interproximal contacts are situated progressively more gingivally from the central incisors to the distal of the canines.
IV- Incisal Embrasures: These become progressively larger from the central incisor to the lateral incisor and canine, contributing to a youthful smile; they become minimal with age and wear.
3- The Nature of Light and Color
A- Light: It is described as the visible electromagnetic energy spectrum, with wavelengths measured in nanometers (nm).
I- The human eye is sensitive only to wavelengths between 380 and 750 nm.
II- Shorter wavelengths include ultraviolet, X-rays, and gamma rays; longer wavelengths include infrared radiation.
III- Pure white light passing through a prism is refracted and separated into colors (Red, Orange, Yellow, Green, Blue, Violet).
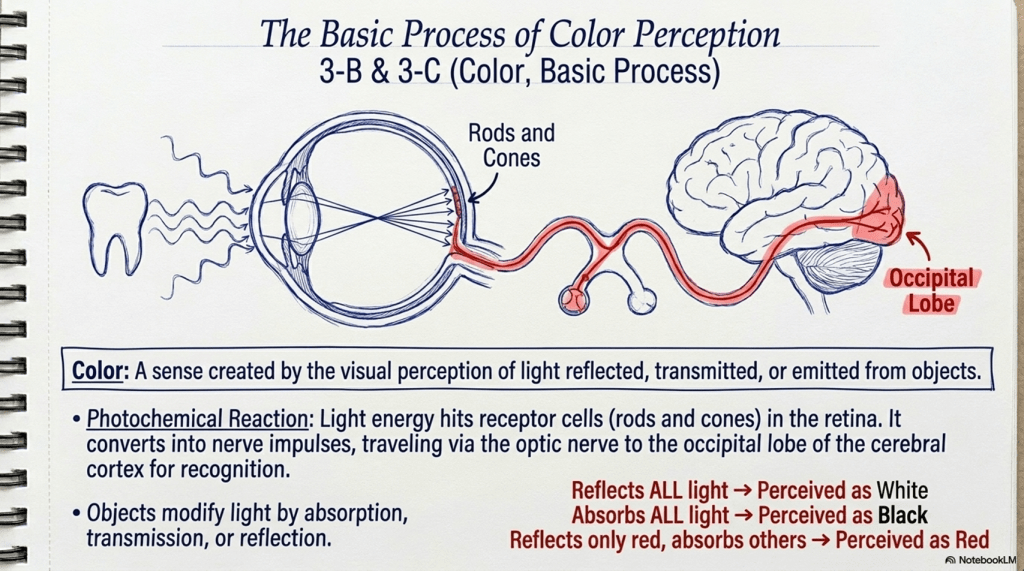
B- Color: It is a sense created by the visual perception of light reflected, transmitted, or emitted from various objects.
I- Visual Perception: Reflected light is perceived by receptor cells (rods and cones) in the retina.
II- Photochemical Reaction: Light energy is converted into nerve impulses, carried via the optic nerve to the occipital lobe of the cerebral cortex for recognition.
C- Basic Process of Color Perception:
I- Objects modify light by absorption, transmission, or reflection.
II- An object that reflects all light is perceived as white.
III- An object that absorbs all light is perceived as black.
IV- An object reflecting only red wavelengths while absorbing others is perceived as red.
4- Optical Properties of Teeth and Materials
A- Translucency: It is the property of a material that partly allows light to pass through.
I- Incisal edges of natural teeth are translucent; in younger patients, incisal enamel is thick and highly translucent.
II- As translucency increases, the value (brightness) decreases.
B- Transparency: The property of a material that completely allows light to pass through.
C- Opacity: The property of a material that does not allow light to pass through; all light is absorbed, and if completely opaque, the color black is perceived.
D- Fluorescence: It is the process where a material (like a tooth) absorbs ultraviolet light energy and re-emits it in a longer, visible wavelength.
I- This emission ceases immediately upon removal of the light source.
II- Fluorescence intensity is three times greater in dentin than in enamel due to organic matter.
E- Opalescence: The phenomenon where a material appears blue in reflected light and red-orange in transmitted light.
F- Metamerism: It is the phenomenon where two objects appear to be the same color under one light source but different under another.
G- Isomeric Pair: Two objects that appear identical in color under all light sources.
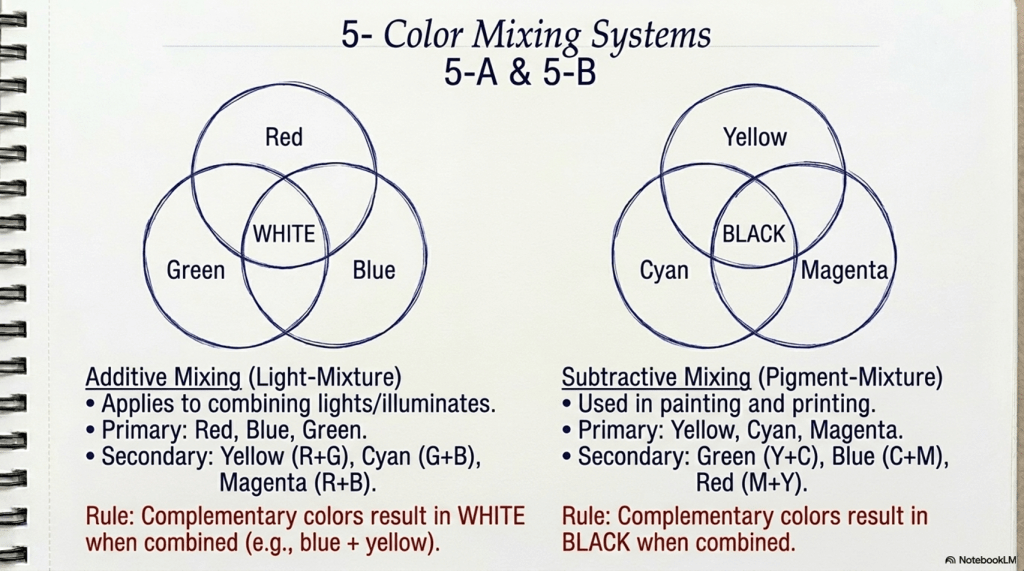
5- Color Mixing Systems
A- Additive Color Mixing (Light-Mixture): This system applies to combining lights and illuminates.
I- Primary Colors: Red, Blue, Green.
II- Secondary Colors: Yellow (Red + Green), Cyan (Green + Blue), Magenta (Red + Blue).
III- Complementary Colors: Two colors that result in white when combined (e.g., blue is complementary to yellow).
B- Subtractive Color Mixing (Pigment-Mixture):
This system is used in painting and printing.
I- Primary Colors: Yellow, Cyan, Magenta.
II- Secondary Colors: Green (Yellow + Cyan), Blue (Cyan + Magenta), Red (Magenta + Yellow).
III- Complementary Colors: Two colors that result in black when combined.
6- Color Description and Order Systems
A- Munsell Color Order System: A visually descriptive system describing color in three dimensions: Hue, Chroma, and Value.
I- Hue: The color itself (e.g., red, green). It is arranged in a wheel of 10 gradations. Most natural teeth fall between yellow and yellow-red.
II- Chroma: The intensity, saturation, or strength of a hue. It ranges from 0 (achromatic/gray) to 14. Natural teeth range from 0 to 7.
III- Value: The degree of lightness or darkness (brightness) of an object. It ranges from 0 (black) to 10 (white). Natural teeth range from 4 to 8.
IV- Designation: Formulated as HV/C (e.g., 5R 4/14).
B- CIELAB Color System: A quantitative system using three coordinates (L*, a*, b*).
I-: Indicates lightness, ranging from 0 (black) to 100 (white).
II-: Represents the red-purple/blue-green axis.
III-:Represents the yellow-purple/blue axis.
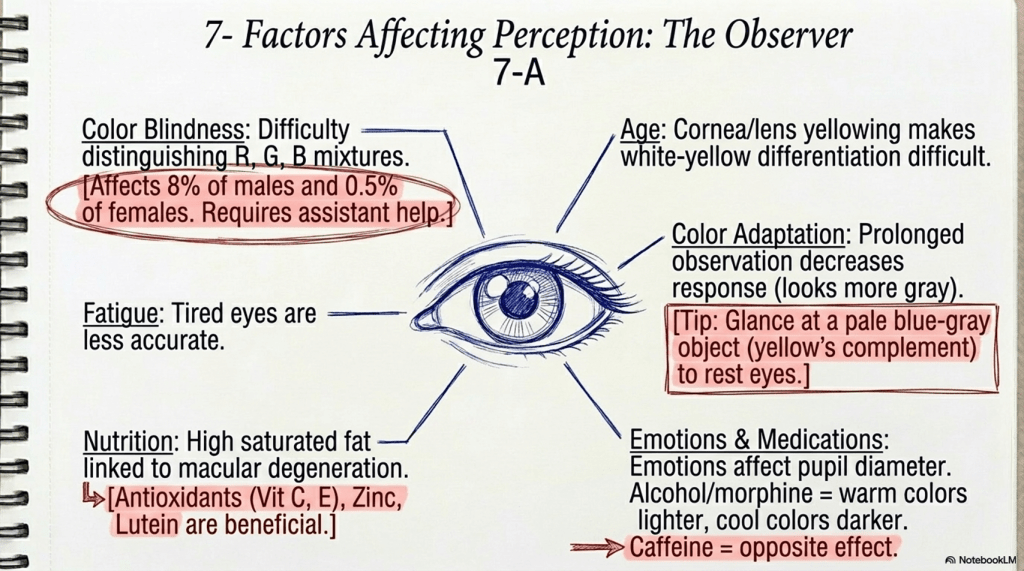
7- Factors Affecting Color Perception
A- The Observer:
I- Color Blindness: Difficulty distinguishing red, green, blue, or their mixtures. Affects 8% of males and 0.5% of females. Assistant help is required if a dentist is deficient.
II- Age: The cornea and lens become yellowed, making white-yellow differentiation difficult.
III- Fatigue: Tired eyes are less accurate.
IV- Color Adaptation: Prolonged observation of a color decreases the response to it (it appears more gray). One should glance at a pale blue-gray object (complementary to yellow) to rest the eyes.
V- Nutrition: High saturated fat intake is linked to macular degeneration; antioxidants (Vitamins C, E), Zinc, and Lutein are beneficial.
VI- Emotions and Medications: Emotions affect pupillary diameter. Alcohol and morphine make warm colors appear lighter and cool colors darker; caffeine has the opposite effect.
B- The Object: Color perception depends on the molecular structure, density, size, and surface texture of the object.
C- The Light Source (Illuminants):
I- Northern Daylight: Best performed between 10 AM and 2 PM on a bright day. Ideal color temperature is 5500 K with a Color Rendering Index (CRI) near 100.
II- Incandescent Light: Higher in yellows/reds, lower in blues, and has a low CRI.
III- Fluorescent Light: Higher in blue energy, lower in reds (CRI 50–80).
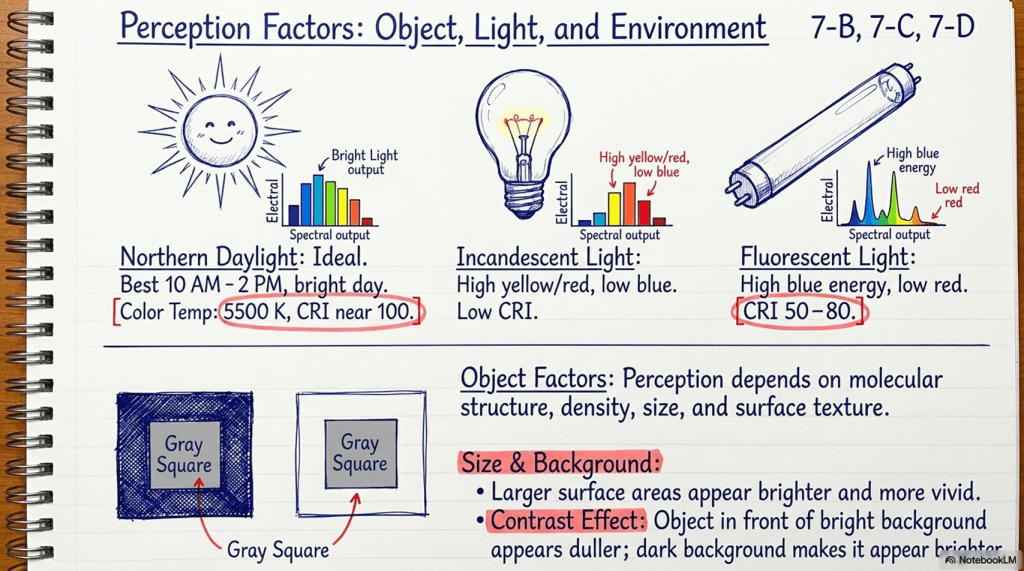
D- Size and Background Differences:
I- Colors covering a larger area appear brighter and more vivid.
II- Contrast Effect: An object in front of a bright background appears duller; a dark background makes it appear brighter.
8- Principles and Techniques of Shade Selection
A- General Principles:
I- Environment should be neutral (walls/cabinets in gray or pastel colors). II- The patient should be upright with teeth at the operator’s eye level. III- View from a distance of 30 cm (normal conversational distance). IV- Perform selection at the start of the visit before teeth dehydrate (dehydration increases Value). V- Remove all distractions (lipstick, bright clothes, large jewelry). VI- Clean and moisten the teeth and shade tabs.
B- Selection Sequence:
I- Observations must be quick (5 seconds or less) to avoid retinal fatigue.
II- Standard sequence is Value, then Chroma, then Hue.
III- Use half-closed eyes to increase the ability to match Value (this decreases color discrimination but highlights brightness).
IV- Divide the tooth into three regions: cervical, middle, and incisal; match each independently.
C- Custom Shade Distribution Chart:
I- Used to record specific characterizations like hypocalcification, craze lines, internal stains, and translucency patterns.
II- This detailed information must be transferred to the laboratory work authorization.
9- Commercial and Digital Shade Guides
A- Visual Shade Guides:
I- Vita Classic (Vita Lumin Vacuum): 16 tabs arranged by Hue (A: red-yellow, B: yellow, C: gray, D: red-yellow-gray).
Within groups, Chroma increases from 1 to 4. A value-oriented sequence (B1, A1, B2…) is recommended.
II- Ivoclar Vivadent Chromascop: 20 tabs in five hue groups (100–500), with Chroma increasing from 10 to 40.
III- Vita 3D-Master: Scientifically based on Value. 26 tabs in 5 Value levels.
Next, Chroma is chosen (M group), and finally Hue (L for yellowish, R for reddish).
B- Digital Shade Matching: These devices eliminate subjectivity and depend on the CIELAB system.
I- Colorimeters: Measure absorbance of wavelengths by comparing against a reference (e.g., ShadeEye–Shofu).
II- Spectrophotometers: More sophisticated and expensive; they include a light source, a means to receive reflected light, and a spectrometer to measure wavelength intensity.
10- Clinical Integration and Communication
A- Trial by Fire (Provisional Restoration): When original tooth positions are lost or significant changes are made for esthetics, the new position must first be tried in a provisional restoration.
I- Patient satisfaction is influenced by feedback from friends and family away from the office.
II- Only after the provisional has passed this “trial” should changes be incorporated into the definitive restoration.
B- Laboratory Communication: Successful results require a team approach. Feedback (positive and negative) and precise prescriptions including diagrams and photographs are essential.
C- Informed Consent: The dentist must inform the patient of the disadvantages of ceramic materials (greater reduction, fracture risk, abrasion) to secure truly informed consent.
D- Disinfection: Shade guides must be disinfected after use; avoid autoclaving as most parts are plastic and heat-sensitive.